

Australians reside longer, but we’re also living longer as a consequence of disease and disability. Half of us now suffers from a minimum of one chronic disease.
As the variety of illnesses increases, the demand for health care increases. In the 40 years since Medicare began, the typical variety of primary care physician visits per person has increased by over 60%.
Today, general practice – where most individuals first go for check-ups, diagnosis and ongoing management of chronic conditions – is under pressure. In 2024 almost 30% Australians said they waited too long to get the essential care they needed.
But Australia does more nurses per person than many similar countries. Removing barriers that prevent nurses from using all their skills could help meet the growing demand for care.
Nurses’ skills are wasted
Primary care works best when it’s delivered by a team: physicians working with nurses, pharmacists, allied health professionals and other health care professionals.
When a team can safely use all of their skills and training, advantages for patients from improved access, equal or higher health outcomes, increased efficiency and potential savings.
However, GPs in Australia are less likely than in similar countries, delegating tasks reminiscent of vaccinations, routine health checks and health promotion to nurses.
The last two independent reviews found that although many practices employ a nurse, most don’t utilize all of their skills.
Grattan Institute, CC BY
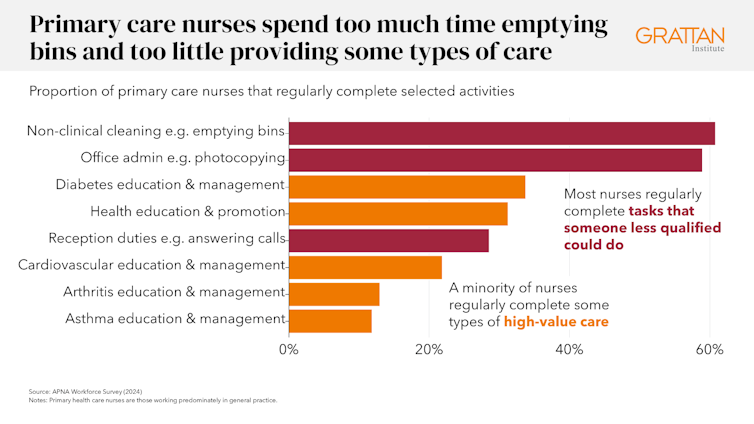
Primary care nurses agree. 2024 labor force survey showed that just one third of surveyed nurses on the whole practice often work to the total extent of their occupation.
Nurses spend an excessive amount of time performing basic tasks that might be performed by others, taking them away from providing the care they’re trained to offer. About 60% of nurses surveyed said they often empty trash bins or make photocopies.
However, despite this, lower than one third often provided health education and promotion services to patients good evidence that it’s secure and effective.
Grattan Institute, CC BY
Nurses want more. Four in ten said they wanted to offer more health education and promotion services.
Nearly half (48%) said that they had asked to perform more complex clinical activities or expand their role previously 12 months.
Although we still have a protracted strategy to go, some progress has been made. The percentage of primary care nurses who said they often practice their full scope of practice increased from 29% in 2019 to 35% in 2024.
Nurses can do more
Over the past 12 months and a half, reviews commissioned by the federal government have identified three key areas for reform.
First, the 12 months 2024 Scope of practice review found industry-wide confusion about what nurses can do and inconsistent state-to-state policies that make it difficult for practices to effectively employ nurse staff.
He called on federal and state governments to create a national framework that clearly outlines what different health care staff can do.
Second, governments and accreditation bodies must change the way in which they regulate health care staff. Regulations should reflect the activities that healthcare staff are trained and qualified to perform safely, fairly than rigid skilled boundaries.
State governments should harmonize their laws – including drugs and poisons laws – in order that rules are tailored to staff’ capabilities and consistent across jurisdictions.
October saw a significant step forward in expanded and nationally consistent nursing roles. Now this will probably be done by specially qualified registered nurses prescribe medications.
An amendment to financing can be needed
Both Scope of practice review and 2024 A review of incentives for general practice found that such changes won’t take full effect without one other change: fixing the way in which Australia funds primary health care.
One example is latest rules allowing medications to be prescribed by a registered nurse. Just last week, the Senate committee voted unanimously recommended Nurse prescriptions needs to be subsidized at the identical pharmacy as prescriptions issued by doctors, as a substitute of costing greater than private prescriptions.
Medicare funding also needs to maintain up. In the present fee-for-service model, healthcare professionals pay for the number and kind of services they supply. This limits the care provided by nurses 3 ways: :
- many services provided by nurse practitioners don’t have a Medicare item number
- for those who do, the payments are sometimes too low to be profitable
- rules require excessive supervision by the physician, which creates inefficiency.
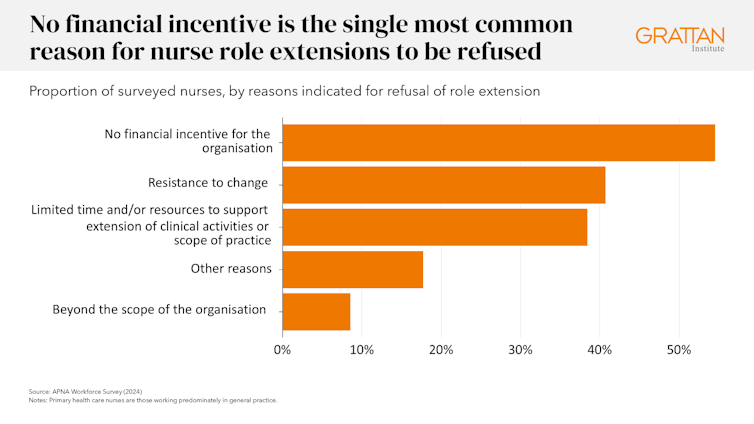
The biggest obstacle to unlocking team-based care is outdated funding rules. Among the surveyed nurses who applied to expand their role and were refused, essentially the most common reason was the shortage of economic incentives for the clinic.
Grattan Institute, CC BY
The Scope of Practice Review also found that healthcare professionals working in fee-for-service settings face the best barriers to using the total range of services, while healthcare professionals working in facilities using more flexible funding models face the least barriers.
The solution is a blended financing model
Under mixed financingGeneral practices can be paid a lump sum to oversee ongoing patient care, with higher payments paid to patients with more complex needs.
This would amount to service fees for individual consultations and procedures.
More flexible funding would allow clinics to determine how best to deliver care, including when nurses should provide it.
Most countries with health systems just like ours already use blended financing, which has been supported by each recent reviews.
The health needs of Australians have gotten more complex and GPs cannot meet them alone. Australia has a big, trustworthy and highly qualified nursing workforce. Governments should act now to remove the financial and regulatory barriers holding them back.





















